
What
The surgery for rectal cancer is more challenging than the one for colon cancer. Particularly lower rectal cancer when cancer is close to the anus or anal sphincter, multidisciplinary treatment team leading by a specially trained colorectal surgeon like Prof. Art Hiranyakas, MD., PhD., has been proven as the most appropriate approach to achieve the best possible outcomes. Anal sphincter is a round group of muscles wrapping around the anus. It functions as to generate the perfect bowel control. Traditional surgery for the patient who has rectal tumor/growth in close proximity with the anal sphincters may require the removal of anal sphincters. The patient would have stoma opening on the abdominal wall for life. The stoma is covered by pouch that will collect the stool from the bowel. The patient will need to empty the pouch from time to time.
When
Patient who has rectal cancer next to the anal sphincters may require a trailer surgical plan in order to achieve both the complete removal of the cancer and anal sphincter preservation. The surgical treatment options for rectal cancer includes
- Transanal local excision (or trans-anal endoscopic microsurgery, TEMS)
- Low anterior resection
- Ultralow anterior resection (with or without trans-anal total mesorectal excision, TaTME)
- Abdominoperineal resection
- Pelvic exenteration
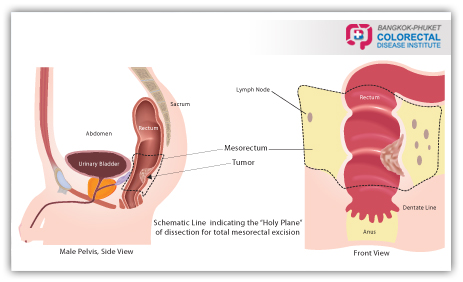
Depending on the stage of the disease, sphincter saving treatments may include surgery alone or the combination of surgery, chemotherapy and radiotherapy. An accurate pre-surgery staging plays a critical role in an adequate treatment planning for each individual. The comprehensive and the most recent pre-surgery staging technology includes Trans-rectal/Endorectal Ultrasonography (ERUS), Magnetic Resonance Imaging (MRI), and Positron Emission Tomography scan (PET-CT scan). Based on the results of pre surgery staging, early stage cancer can be treated with trans-anal local excision/TEMS when no surgical incision on the abdominal wall is required. This surgical technique could be performed through the anus using special designed surgical instruments by experienced colorectal surgeron. Most of the larger low rectal cancer could also be treated with colo-anal anastomosis to avoid a permanent stoma. Furthermore, the standard of surgical care is to perform a total mesorectal excision (TME) procedure. This will involve the removal of the rectum together with the surrounding envelop of lymph nodes.
Why
 The most challenging surgical treatment for all colorectal cancer patients is when the tumor is located in an area very low in the rectum o close to anal sphincters. The general surgeon most of the time offers to remove both rectal tumor and the anus for this group of patients. However if the anus is removed, the patient will typically need a permanent stoma. Sphincter sparing surgery is the surgery that is performed by a specialized colorectal surgeon to avoid the removal of the anal sphincters. The preservation of nearby nerves is also essential for this surgical procedure to maintain normal post-surgery bowel, bladder, and sexual function. The combination of advanced technologies may be required to preserve the sphincter whenever possible. Because of the inconvenience of the stoma, colorectal surgeon offers sphincter saving treatments that allow the rectal cancer patient to preserve the function of the anus. The surgery may be performed through the abdomen or the anus (using trans-anal total mesorectal excision, TaTME) or the combination of the abdominal and the anal approach. The advances in surgical technologies and techniques are nowadays allowed the specially trained surgeon to perform the sphincter saving surgery using laparoscopic/key-hole surgery or even the robotic assisted surgery.
The most challenging surgical treatment for all colorectal cancer patients is when the tumor is located in an area very low in the rectum o close to anal sphincters. The general surgeon most of the time offers to remove both rectal tumor and the anus for this group of patients. However if the anus is removed, the patient will typically need a permanent stoma. Sphincter sparing surgery is the surgery that is performed by a specialized colorectal surgeon to avoid the removal of the anal sphincters. The preservation of nearby nerves is also essential for this surgical procedure to maintain normal post-surgery bowel, bladder, and sexual function. The combination of advanced technologies may be required to preserve the sphincter whenever possible. Because of the inconvenience of the stoma, colorectal surgeon offers sphincter saving treatments that allow the rectal cancer patient to preserve the function of the anus. The surgery may be performed through the abdomen or the anus (using trans-anal total mesorectal excision, TaTME) or the combination of the abdominal and the anal approach. The advances in surgical technologies and techniques are nowadays allowed the specially trained surgeon to perform the sphincter saving surgery using laparoscopic/key-hole surgery or even the robotic assisted surgery.